Both Sides of the Breakthrough: Kelly Stevens
As a patient, she's lived what biomedical engineering can do. As a researcher, she's building what comes next.
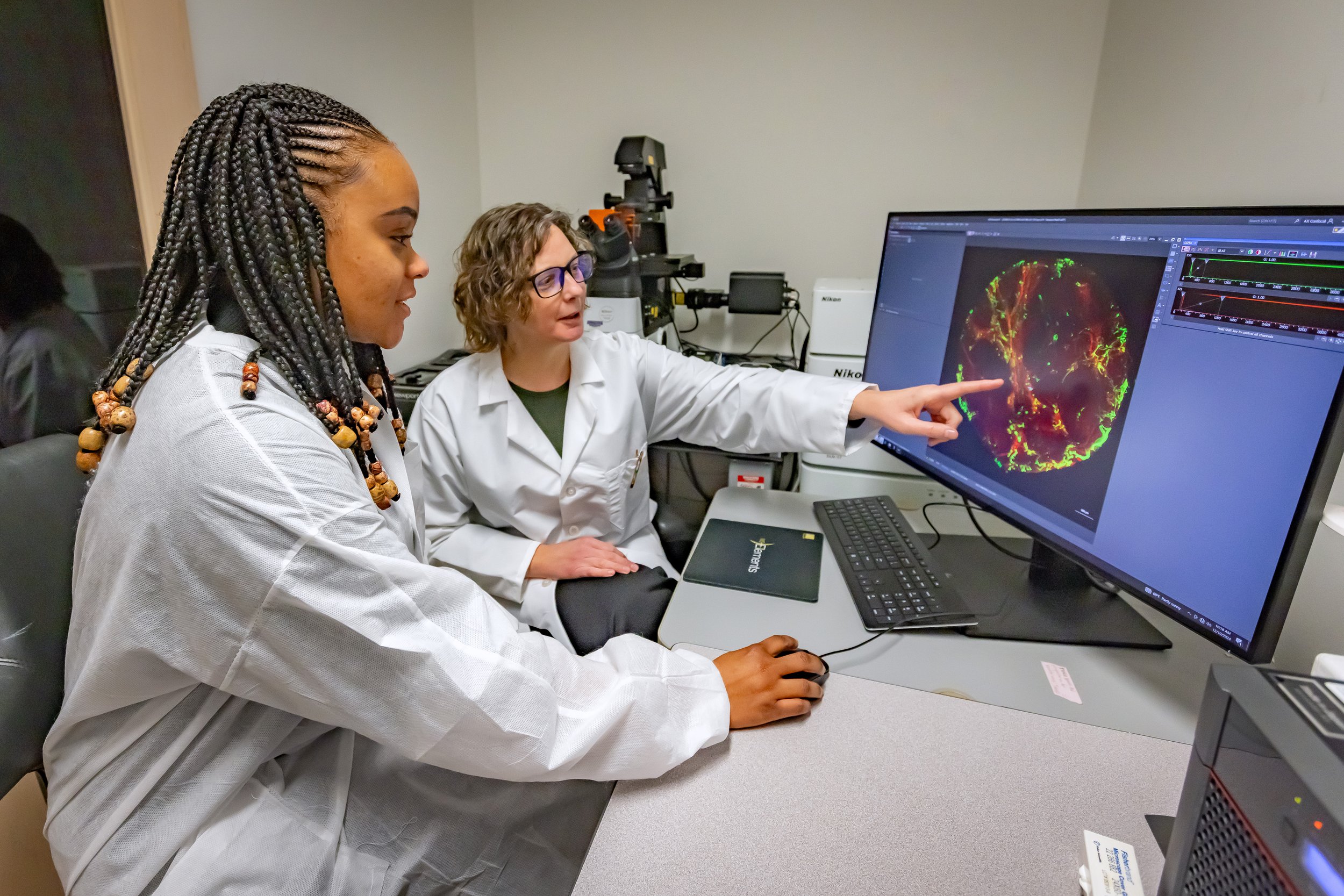
Kelly Stevens, right, looking at image of the blood vessels in human liver on a computer | Photo credit: UW Medicine.
At scientific conferences, colleagues know Kelly Stevens, Ph.D., by her seat cushion. She carries it everywhere, and she'll tell you why.
If it weren't for the drugs she's been taking since college, she wouldn't be able to walk at all.
This is not typically how you'd introduce one of biomedical engineering's most decorated researchers. Stevens is an Associate Professor at the University of Washington, recipient of the BMES 2024 Mid-Career Award — the highest honor the field gives at that career stage — and the scientist leading a lab that is, not metaphorically but literally, building human organs from stem cells. She is at the frontier of what biomedical engineering can do.
She's also someone who has depended on biomedical engineering's continued advances her entire adult life.

Kelly, growing up in northern Wisconsin | Photo credit: Cathy Stevens
From New Richmond
Kelly grew up in New Richmond, Wisconsin, a town of then about 5,000 people that's an hour and a half outside of Minneapolis. Her family was comprised of construction workers, farmers, and nurses. "If you're from a small town, you don't even know what a scientist is," she says. As a kid, she thought she'd be a doctor or nurse because those were the only person she knew who worked with the human body.
She also grew up with psoriasis. It started around age 10, and at its worst covered roughly 70% of her body — arms, legs, stomach, back, scalp. "Imagine the worst eczema you've ever seen," she says. "I had it really bad."
The treatments available then weren't much. Steroid creams that helped a little. And UV light therapy, administered in a clinical setting but, as Kelly puts it, "basically a tanning bed." Her doctors in college told her with a straight face: this is your treatment, and you're probably going to get skin cancer from it.
She learned to manage.
A Revolution in a Drip Bag
Then, during college at the University of Wisconsin–Madison, one of her toes swelled dramatically. It ballooned into what is called a "sausage digit" — the description is literal. She went from doctor to doctor trying to find an explanation. Five doctors in, someone finally connected it to her psoriasis: she had psoriatic arthritis, an autoimmune condition where the immune system attacks the body's own joints. The diagnosis was unwelcome, but it put her on a path that would change her life.
Her rheumatologist told her about a new drug that had just been approved — one of the first of an entirely new class called biologics. Rather than broadly suppressing the immune system, biologics work with precision. They find a specific signaling molecule that's misfiring and block it.
In Kelly's case, that molecule was TNF alpha, which was triggering her immune system to attack her own body. The drug, Remicade, was delivered by IV infusion: a four-to-five-hour clinic visit every several weeks. Her doctor thought it might help the arthritis. He mentioned as an aside, that it might do something for the psoriasis that she’d been grappling for over a decade, too.
Two days after her first infusion, Kelly's psoriasis was gone.
Not better. Gone.
"It went from covering my arms, my legs completely, my stomach, my back, my head. And literally two days later, it was just snap gone," she recalls.
She made an appointment with her dermatologist specifically to show her. Something that had defined her since childhood had disappeared because researchers had figured out what was going wrong at the molecular level and engineered a solution.
That was more than two decades ago. She eventually became one of those researchers — and her experience as a patient has never been far from the work. Today her lab at UW focuses on engineering synthetic human tissues from stem cells, with the goal of building replacement organs and translating that science into real therapies. It's research shaped, at least in part, by a lifetime of understanding what it costs when the body turns on itself.

Kelly, fishing in northern Wisconsin just after her psoriasis cleared! Photo credit Cathy Stevens
Running Out of Road
The story isn't simple, though. Biologics have limits. The body is adaptive. Over time, it finds ways around the block. The drug stops working. You move to the next one.
Kelly is now on her ninth, the last currently available in her treatment pipeline. Her arthritis hasn't gone away. She walks slowly and carries her seat cushion. She can't run or bike or climb mountains the way she once did.
"If it weren't for these drugs, I wouldn't be able to walk," she says. And she knows this from experience. When she's late for a dose, she feels it immediately.
The Invisible Thread
During graduate school, Kelly was introduced through her university to a potential donor — a man whose company she hadn't yet looked up. When she learned he had founded the first company to treat her condition, she started crying on the spot. "You changed my life," she told him.
That's the invisible thread biomedical engineering weaves between researchers who will never meet their patients and patients who will never know the names of the people who helped them. Kelly lives on both sides of that thread, every day.
She holds both realities at once: the frustration of a patient running out of options and the hard-won optimism of someone who has watched a field completely reimagine what's possible within a single lifetime.
"As a patient, I can say we're not there yet. I still have a lot of really hard days. But then I see what my colleagues are doing, and there's so much our field is on the verge of fixing. The medicines that are coming soon work better, will be adapted for each patient, and won’t require me to carry my medicine on ice everywhere I go. For the first time in my life, it is even possible they will eventually offer full cures.
That makes me grateful and hoping our science endures to make this progress. It is very personal for me because my 10-year-old daughter was just diagnosed with my disease. If our field keeps innovating, she will be able to grow up with a lot less pain — both physical and emotional — than I have. We've learned so much just in a couple of decades, and we are on the cusp of so much more," she says.
She knows what it looks like when new scientific breakthroughs arrive. She's been waiting for it, and building toward it, her whole life.
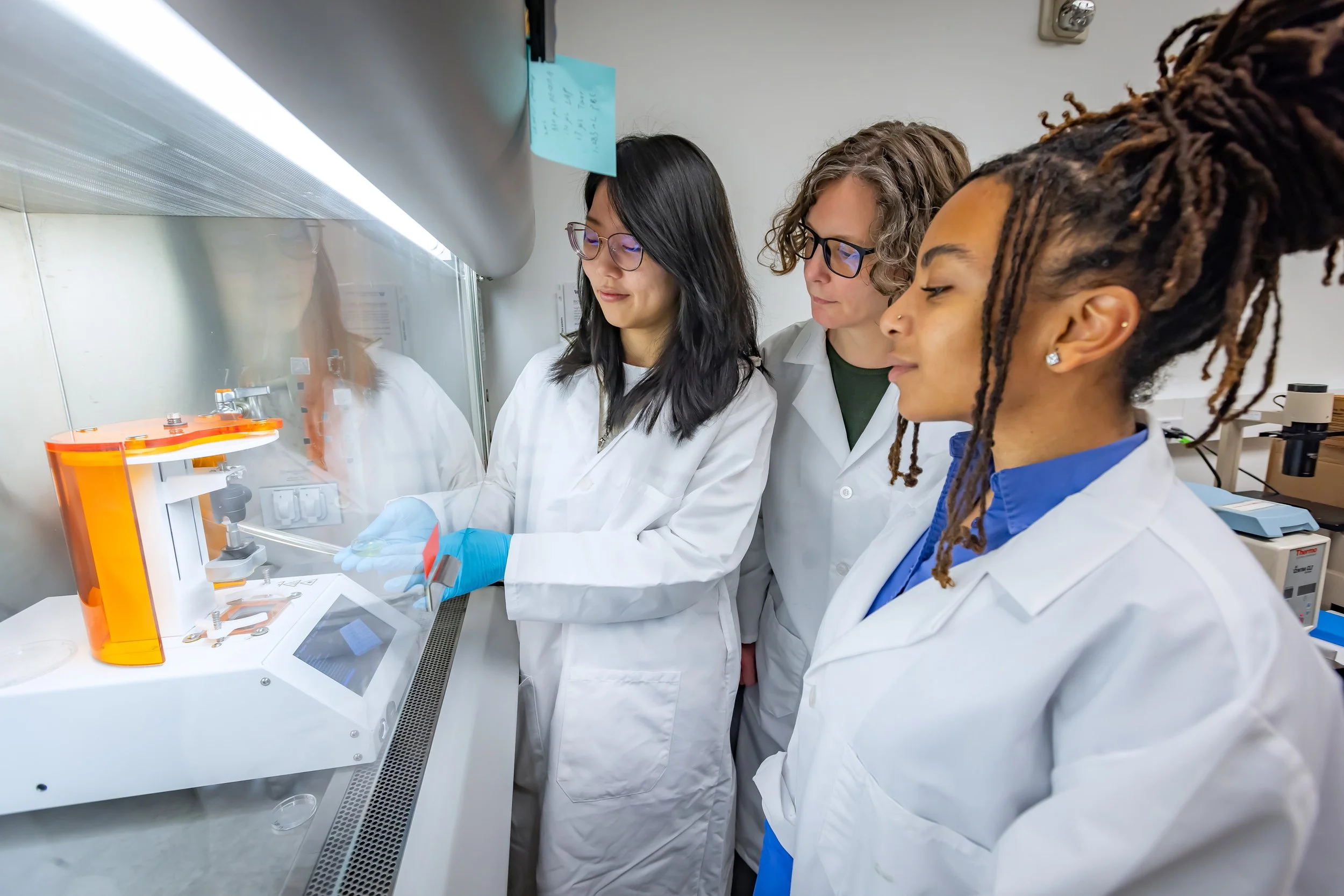
Kelly Stevens, middle, working with an organ bioprinter. | Photo credit: UW Medicine.